Epidemiology
by Wade. H. Frost
Epidemiology is defined in authoritative works of reference as "the science or doctrine of epidemics," and this or some equivalent statement is the only definition which is etymologically correct. This definition implies, however, that the phenomena of epidemics are distinct from those of the interepidemic or endemic occurrence of disease; and though such a view appears actually to have been held in former days, it is now recognized that an epidemic is only a temporary phase in the occurrence of any disease, and that its phenomena cannot be considered scientifically except in relation to the antecedent and subsequent history of the disease. Consequently, usage has extended the meaning of epidemiology beyond its original limits, to denote not merely the doctrine of epidemics but a science of broader scope in relation to the mass-phenomena of diseases in their usual or endemic as well as their epidemic occurrences. Although it is clear from current usage that the definition of epidemiology has been thus extended beyond its original sense, it is not clear just how far it has been extended. It is certain that its scope is not usually limited to the diseases in which epidemics are characteristic, since it is entirely in conformity with good usage to speak of the epidemiology of tuberculosis; and it seems customary also to apply the term to the mass-phenomena of such non-infectious diseases as scurvy, but not to those of the so-called constitutional diseases, such as arterio-sclerosis and nephritis. Therefore, in view of the latitude which the uncertainty of usage allows, epidemiology will be considered here as referring exclusively to the diseases of man which are classed as specific infections, since this will permit of a more coherent discussion.
In this sense epidemiology may be defined as the science of the mass-phenomena of infectious diseases, or as the natural history of infectious diseases; or it may be more fully described in the terms which Hirsch applies to the science which he calls historical and geographical pathology, as "a science which . . . will give, firstly, a picture of the occurrence, the distribution and the types of the (infectious) diseases of mankind, in distinct epochs of time and at various points of the earth's surface; and secondly, will render an account of the relations of these diseases to the external conditions surrounding the individual and determining his manner of life." 1 As is implied in this statement, epidemiology is essentially an inductive science, concerned not merely with describing the distribution of disease, but equally or more with fitting it into a consistent philosophy.
1 This definition is deficient in that it fails to take account of variations in the inherent traits of individuals as factors in the distribution of disease; but the statement is otherwise so admirably expressed that it is quoted without attempt to amend it.
The Data and Scope of Epidemiology.—For the clinical description of a disease the unit is an individual, and the phenomena of the clinical reaction may be described in terms of the character and distribution of anatomic lesions and the nature and sequence of symptoms. For epidemiological description the unit is an aggregation of individuals making up a population, and description of the mass-phenomena of a disease consists of a statement of its types and frequency of occurrence in the population as a whole and in its different component groups. As compared with the clinical manifestations of a disease, its epidemiological characteristics, which can be put together only in a conceptual way, are more difficult to comprehend but not less distinctive. For example, given sufficient opportunity for direct observation, it is comparatively easy to form a clear clinical picture of such a disease as typhoid fever, and to contrast this picture sharply with that of another disease as different, say, as measles. In each of these diseases one may readily observe a quite distinctive character and distribution of physical signs and symptoms, and, continuing the observations from day to day, may note, by such objective signs as temperature, rash, facies, and demeanor of the patient, the very different courses which the two diseases run.
It is much more difficult to form equally clear mental pictures of these diseases in terms of their different distributions in a large population; that is, of their differences in selection of certain elements of the population in relation to various features of environment and in varying trends of prevalence from year to year or from month to month. Nevertheless, when these epidemiological features of any disease have been adequately determined and described, they are found to be definitely distinctive. It is found, for instance, that measles selects almost exclusively those people who have not previously had this disease; that (largely because of this circumstance) it falls chiefly upon children; and that, in a large proportion of the households invaded, two or more cases have occurred in fairly close sequence. Typhoid fever will be found to have selected individuals of quite different age distribution, without respect to whether or not they have previously had measles, but usually sparing those who have previously had typhoid fever; and it will usually show a distribution which is demonstrably selective for those classes of the population that are least protected against excremental contamination of their water and food. If the records for a series of years are examined, the two diseases will be found to have run quite different courses as regards seasonal distribution and range of oscillations in prevalence from year to year. These and many other features of distribution, which could be demonstrated by a full analysis of the population and adequate morbidity records, would establish, for each disease, a set of epidemiological characteristics just as distinctive as its clinical characteristics and serving equally well, if the description were adequate, to differentiate it from other diseases.
Merely to describe a disease in such terms as have been indicated above requires the collection, from many different sources, of facts which, if considered separately or in a different combination, would be classed as pertaining to some other science than epidemiology. Hence, notwithstanding that epidemiology is a sufficiently distinct science with respect to the character and coherence of its data, it is essentially a collective science, and its progress is largely dependent upon that which has been made in other fields. For example, since description of the distribution of any disease in a population obviously requires that the disease must be recognized when it occurs, the development of epidemiology must follow and be limited by that of clinical diagnosis, and of the rather complex machinery required for the systematic collection of morbidity and mortality statistics. Epidemiology must also draw upon statistical method and theory, because even the simplest of quantitative descriptions must be stated statistically; and more minute descriptions, involving perhaps the demonstration of complex associations, may require the application of quite elaborate statistical technique. Moreover, quantitative epidemiological descriptions, in terms of the frequencies of diseases in different population groups, require, as part of their data, more or less detailed statistics of population, implying the prior development of demography; and for descriptions of the relations of disease to climate and weather, systematic meteorological records are necessary.
To all of the data which can be collected from fields which are cultivated primarily for other purposes, it is usually necessary, for more detailed descriptions of the mass-phenomena of diseases, to add another set of facts collected especially because of their epidemiological significance. These, which are, perhaps, the most distinctive data of epidemiology, include systematic collective observations on the incidence of different diseases in relation to such details of local environment, personal habits, past history, and individual traits as may be supposed to have a probable relation to the occurrence of the diseases. Observations of this kind, which are necessary for establishing some of the most fundamental characteristics of diseases, such as the relation to contact with a prior case, the degree and duration of immunity, etc., are of especial importance for the guidance and evaluation of preventive measures, and are discussed more fully later in that connection. They are usually procurable only for samples of population, and may usually be collected most conveniently by administrative public health organizations.
All the above discussion refers only to such data as are necessary for descriptions of diseases. However, epidemiology is never, in fact, developed as a purely descriptive science. In collecting facts about the distribution of disease, the purpose in view is always to arrive at a better understanding of its nature, sources, means of spread, and eventually its control. This implies that the facts must be related to each other in such an orderly way as to establish a theory or philosophy of the disease; and, as this theory must be consistent with all the accepted principles of the broader natural philosophy into which it is fitted, epidemiology must come into relation here with the whole field of natural science, but more especially that of biology. With respect to a specific infectious disease, any theory of its epidemiology must take into account the facts known from direct observation of the specific microorganism if this has been identified; and must, in any case, be consistent with the general facts known about the class of organisms to which the specific infective agent is assigned.
Hence, for the explanation of the observed distributions of disease, epidemiology, as a constructive science, must draw a large and important part of its data and principles from the related sciences of pathological bacteriology, protozoology and immunology. In fact, epidemiology must either be considered broadly as including these sciences or, if more narrowly defined as distinct from them, it may be conceived as an extension from the opposite side into a field where most of the ground is in common. In explanation of the relation thus described, since an infectious disease is considered to represent a reaction in which at least two separate organisms are concerned, the human host and the infecting microorganism, there are two principal approaches to the development of a theory explaining the distribution of the disease. One approach begins with observations of individual cases as they occur in nature, noting, in each case, certain attendant or antecedent conditions and circumstances, and proceeds inductively, by the accumulation of observations, to build up a chain of associations between the occurrence of the disease and certain related conditions and combinations of circumstance. If the specific microorganism has not been identified and experimentally established as the causative agent, its existence and certain of its essential characteristics may be inferred from such circumstantial evidence. If the specific infective agent has been experimentally established, observations of this kind often lead to the inference of certain of its characteristics which have not been experimentally demonstrated. The other approach begins with direct observation of the specific microorganism itself, ascertaining something of its actual distribution in nature and of its reactions under controlled experimental conditions. From these observations inferences are drawn by an essentially deductive process as to the life history and behavior of the microorganism under the more complex conditions of nature. It may well be, as in the case of malaria, that this approach furnishes the clue to an interpretation of facts which the other approach had discovered but not explained.
The distinction which is made here as between the inductive and the deductive method is only a general one which cannot be made consistently ; for whether investigation is started from one side or the other, it advances by a process of alternating induction and deduction, observation leading to hypothesis and this again to further purposeful observation for verification or correction of its formula. Therefore, the real difference which has been illustrated is in the direction from which the approach is made rather than in the method. Actually, investigations starting from the side of descriptive epidemiology are mutually dependent and advance together. Observation of the distribution of an infectious disease in nature suggests a plan for its experimental investigation; and this, if it be fruitful, points in turn to further studies of the natural occurrence of the disease to test and extend the inferences drawn from the experimental evidence. In every case, a combination of the facts and inferences drawn from the two sides extends knowledge more widely and establishes principles more solidly than could be done from either set of data by itself.
It has so happened that in the development of research in recent years the two lines of approach to the problems of epidemiology have been pursued more or less separately, one group of investigators working from the experimental side, in pathological bacteriology, protozoology and immunology, while another group has worked from the side of the actual distributions of infectious diseases in nature. Such specialization has been useful and necessary because of the quite different technical methods which must be employed in the two converging lines of research, but the distinctions which it has established are merely technical differentiations between sections of the same field. Definitions would be less confused if that section of epidemiology which is distinct from bacteriology and protozoology had been given a distinctive name. Since this has not been done, there is a confusing double usage of the term epidemiology, sometimes to designate the whole field and sometimes to designate a special section of it, just as the term pathology is sometimes used in a restricted sense to denote that section of the science which deals specifically with morbid anatomy.
THE DEVELOPMENT OF EPIDEMIOLOGICAL THEORY
The theories of epidemiology which have been recorded more or less definitely in successive ages of the period covered by historical records have been limited in their approach to present conceptions, not merely by the facts known about the characteristics and distribution of disease, but .equally or more by the status of contemporary knowledge and thought in other fields, since this has largely governed the interpretations given to the facts. Therefore, any history of the evolution of epidemiological conceptions, to be at all adequate, must need be, at the same time, a history of the evolution of natural science. Without this background it is impossible to see just what significance would be attached, in a given period, to a given set of facts; and it is at least difficult, or even impossible, in attempting to interpret the theories which are explicitly stated, to distinguish between ideas which are based on mere speculation and those which follow as legitimate inferences from previously accepted principles of natural science. Since no such complete account can be given here, no attempt will be made to trace the development of the theory of infection up to the time when it was finally established on an experimental basis, in the last quarter of the nineteenth century, except to review briefly the farthest progress that had been made up to that time. The two periods thus separated are essentially distinct because, in the latter period, dating from about 1865 to 1875, epidemiological theory has been based firmly on a set of directly demonstrated facts which, in the earlier period, could only be inferred.
Progress Prior to the Establishment of Bacteriology.—By the middle of the nineteenth century the more common and distinctive of the specific infectious diseases endemic in western Europe had been fairly well differentiated clinically. Typhoid fever was still, to some extent, confused with typhus, and scarlet fever with diphtheria, and in various other respects differentiation was less clear than at present; but distinctions not generally recognized were already clearly established in the minds of the keenest observers, and the resultant confusion in epidemiology was probably of less serious importance than it may appear to have been. A good deal was also known, at least in an empirical way, of the epidemiology of the endemic diseases; as, for instance, of their varying mortality in different years and in different places; of the communicability from person to person of the venereal diseases, smallpox, measles and some others of the exanthemata; of the definite immunity conferred by certain diseases; of the association of typhoid and typhus fevers with filth and of malaria with certain localities, etc.
There was also an extensive literature on epidemics, and especially on the epidemics of cholera which had invaded Europe at intervals during the preceding twenty-five or thirty years. As to the epidemiology of such diseases as diphtheria and typhoid fever, which were not generally recognized as being contagious, there were not lacking local studies, such as those of Bretonneau and Gendron, which gave convincing proof of their communicability. Also, as a matter of great importance, it was known that smallpox and vaccinia could be transmitted from person to person by inoculation of a minute amount of pustular matter, and could be propagated in this way through an indefinite number of generations. Similar facts were known about certain epidemic diseases of domestic animals.
Although microbiology had not been established as a science, it was well known that microorganisms were constantly associated with putrefaction and other processes of fermentation. Concerning the life history of these minute organisms, the principle of biogenesis as applied to them was still in dispute; but, on the preponderance of evidence, at least a strong minority of scientists had already accepted this principle as being of general application in biology.
Most of the theories of epidemiology which attempted to interpret these facts were so vague that they could not be put to any scientific test and can hardly be considered as anything more than ingenious hypotheses. There were, however, a few epidemiologists who were able to weave the complex facts into a logical, clear, and remarkably strong inductive argument for a generally applicable germ theory of infection. Of such arguments, that presented by John Snow is perhaps the clearest, most concise, and most direct; and may well serve to illustrate the best epidemiological conceptions of his day.
Snow's most comprehensive statement of his epidemiological theory is given in a brief paper published in 1853 under the title, On Continuous Molecular Changes, More Particularly in Their Relation to Epidemic Diseases. lie begins with a review of general biology which leads up to the principle of biogenesis and acceptance of specific reproduction as a property common and peculiar to living organisms. Prom this he argues that the virus of smallpox, which, on inoculation, will cause the disease and reproduce a vastly greater amount of similar virus, is, in fact, a living organism; and he calls attention to the fact that the properties of this virus resemble those of known living organisms in two other respects, namely, that it may lie dormant, as do seeds and spores and that like them it requires a period of incubation for reproduction of its progeny. Then, referring specifically to '' syphilis, smallpox, erysipelas, yellow fever, plague, cholera, dysentery, influenza, whooping-cough, mumps, scabies and the entozoa," he classes all these as "communicable" diseases, caused by the continuous transfer from person to person of a living virus, visible in the case of the entozoa, invisible in the other diseases. He supports this view by noting that in all these diseases clear evidence of their transference from person to person is demonstrable at times, and that all the circumstances of their occurrence in nature are consistent with the theory that they arise only as the result of such transference from pre-existing cases of the same sort. He shows that a certain proportion of untraceable infections are not inconsistent with his theory, but are a necessary deduction from it; and greatly extends the previous conception of contagion by recognizing water and food as potential vehicles of infection, certainly in cholera and probably in some other diseases.
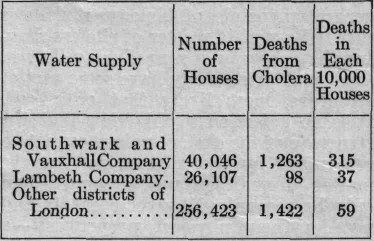
If this paper of Snow's stood alone it might perhaps be considered as only an exceptionally brilliant and happy speculation, since its discussion of infectious diseases, though it is consistent and logical, is quite general and does not attempt a detailed explanation of the epidemiological phenomena of any single disease. A thorough and detailed exposition is given, however, in his treatise on the epidemiology of cholera, published first in 1849, and republished in much more extended form in 1855. In this Snow presents the theory that cholera is a communicable disease, caused by a specific microorganism, multiplying in the human intestinal canal, escaping in the fecal discharges, and transmitted by contaminated food and water. This theory, which is stated as clearly and definitely as it could be stated today, is not only tested against every general fact which was already known about the distribution of cholera, but is scientifically and rigidly tested by observations planned and made by Snow for this particular purpose. It is certain then, that his germ theory of infectious diseases was not a mere speculation but was a logical inference from facts which fully justified his conclusion.
Snow's work is cited not as the only example nor the earliest one of a well-developed theory of the same general import. For long years prior to this period opinion had been tending definitely, though slowly and hesitatingly, to this explanation of the accumulating facts of epidemiology, and certain of Snow's contemporaries, notably Budd in England and Henle in Germany, presented evidence and arguments of great force and clarity. Their writings, together with those of Snow, are sufficient to show that increasingly accurate and extensive observations on the natural distributions of certain diseases, interpreted in the light of broader and more definite conceptions of biology, had already given the germ theory of infection a definite scientific status before it was experimentally established.
Progress Since the Establishment of Experimental Bacteriology.—The evidence accumulated in support of the microbial origin of certain diseases within a few years after Pasteur and Koch had thrown open the doors of experimental bacteriology was so simple, direct, and convincing that the theory gained almost immediate acceptance. It was soon perceived, too, that the germ theory which had been established experimentally for some of the communicable diseases offered such a complete explanation of the general epidemiology of other obviously communicable diseases, such as smallpox, measles, scarlet fever, that the theory of microbial origin was promptly extended to them even though their specific microorganisms remained unidentified. So fundamental was the early work done by the pioneers in bacteriology and the allied sciences that there has been no radical change in the basic epidemiological theory which had been established within two decades by Pasteur, Koch, and their contemporaries. However, in later years there have been some distinct modifications of the views which were held at that period with respect to the importance of different factors in the spread of infectious diseases.
As regards general conceptions of epidemiology the most notable of the advances made in the last three decades have been: (1) demonstrations of the role played by suctorial insects in the conveyance of certain diseases, and as related to this, the part played by some of the lower animals, especially rodents, as reservoirs of infection; and (2) the demonstration that passive carriers of certain specific microorganisms are quite numerous in proportion to the clinical cases. During the first two decades of medical bacteriology, before these two principles had been recognized, attention had been focused almost exclusively upon clinically recognized cases of infectious diseases as the all-important sources of infection, and upon mechanical conveyance as the sole mode of transmission. Consequently some of the most distinctive epidemiological characteristics of certain insect-borne diseases, and of others in which passive germ carriers are common remained without explanation or were disregarded in a forced explanation, based on supposed mechanical conveyance of infectious material direct from recognized clinical cases. From the standpoint of prevention, exaggerated importance was thus attached to the isolation of ill persons and disinfection of their immediate environment.
Still more recently increasing attention has been paid to the frequency and epidemiological importance of sub-clinical infections, resulting in specific immunity. Recognition of this principle has already greatly modified current views of the epidemiology of tuberculosis, diphtheria, scarlet fever, and some other diseases, and promises to lead to a much clearer understanding of the epidemiology of numerous other diseases.
Among developments which cannot yet be appraised in their full significance may be mentioned the work of d'Herelle and others on the bacteriophage in relation to infection and immunity; the gradual accumulation of experimental and circumstantial evidence with respect to variability of the infective power and virulence of certain specific microorganisms; and the beginning that has been made in the quantitative study of epidemics of indigenous diseases in laboratory animals under experimental conditions.
Purposes and Present Importance of Studies of the Phenomena of Diseases in Nature.—Although the most notable contributions to epidemiological theory in recent years have come from experimental investigations, studies of the epidemiology of infectious diseases in nature have continued to contribute an important if inconspicuous share. Such studies are at present necessary chiefly (1) for extending the general theory of the sources and spread of each disease, and (2) for reducing to more specific terms the general knowledge which experimental studies yield concerning the conditions governing the spread of diseases.
To illustrate the first of these general purposes, the transmission of an infectious disease under controlled experimental conditions suffices to prove that all the factors essential to natural transmission are comprised within the more or less narrowly limited conditions of the experiment, but it does not prove the converse proposition, that these are the only conditions under which infection may occur. Such a proposition can be proved only by exclusion, and the nearest approximation to absolute proof is found in the experience that all the observed circumstances of the occurrence of the disease in nature are consistent with the hypothesis that the conditions experimentally indicated actually have been fulfilled in every single instance. Supplementary epidemiological proof is the more essential in proportion as the experimental evidence may be deficient; and in fact, as to a number of diseases which are now accepted as specific infections, the experimental evidence, taken by itself, is by no means convincing; while for a few diseases, such as influenza, the experimental evidence is so uncertain that belief in the agency of a specific microorganism is based principally if not wholly on inference from clinical and epidemiological resemblances to other diseases of demonstrated microbial origin. Again, such knowledge as we possess of the firmness and durability of the immunity acquired by man from an attack of any infectious disease, rests almost wholly on inference from observations on the natural occurrence of the disease.
The general importance of accurate epidemiological observations for extending in more detail the fundamental knowledge based upon experimental evidence is sufficiently obvious. Knowledge of most of the important infectious diseases has already advanced to the point where certain fundamental conditions of their propagation and transmission have been more or less fully established on experimental evidence. Thus, it is usually known whether the specific organisms are propagated in human or extra-human sources, and what general conditions are required for their transmission, whether it may take place by mechanical conveyance of infectious material, or only through the agency of an intermediate host. However, such general knowledge does not suffice for full understanding of a disease or for its most effective prevention, since the broad conditions of transmission may be fulfilled in a number of ways. For example, it is well established that the natural habitat of the typhoid bacillus is the human body, that it is discharged in the intestinal excreta and that it requires only mechanical transmission to the mouth as its portal for establishing infection. The sources are, however, of several classes; namely, clinical cases, convalescents who may be temporary carriers, and other transitory or chronic carriers. Also there are many possible modes of conveyance: by direct personal contact, or indirectly through a third person; by flies having access to excreta and thence to food; by contamination of water; by milk; and in various other ways. From the standpoint of prevention, a knowledge of the relative importance of these various sources and routes is needed; and such knowledge cannot be gained by experiment, but only by careful study of the actual distribution and associations of the disease in its natural occurrence. Moreover, since different sources and routes of conveyance may, and in experience actually do, vary in relative importance in different communities and at different times, local epidemiological studies are a continuing necessity for the effective guidance of control measures.
GENERAL FACTORS WHICH DETERMINE THE DISTRIBUTION OF INFECTIOUS DISEASES
The definition of an infectious disease of man as a reaction between a specific microorganism and a human host implies that for the occurrence of each case of the disease two conditions must be fulfilled, namely: (1) that the specific microorganism must be brought into contact with the human host; and (2) that the reaction which constitutes the disease must follow. The contact, to be effective, must usually be of a special kind; that is, the microorganism must be introduced through some favorable portal of entry, which varies for different microorganisms. This may be conveniently called "effective contact" to distinguish it from essentially impotent contact, such, for example, as simple contact of the tubercle bacillus with the unbroken skin.
Determining Factors.—The distribution of each disease in a population will be determined, therefore, by two sets of conditions; those which govern the frequency and distribution in the population of effective contact with the specific microorganism, and those which govern the frequency with which the disease follows this contact in different classes of individuals and under different circumstances. These two events may be related to each other in many different and complex ways, and each is presumably determined in part by characteristics of the specific microorganism, and in part by characteristics of the population with respect to environment, habits, inherent or acquired immunity, etc. As it is not possible, in any single disease, to analyze fully the complex interplay of these factors, it would be futile to attempt any discussion of them beyond such as may serve to illustrate something of the complexity of even the more obvious influences.
Character of the Essential Reservoirs of Iinfection.—Each specific microorganism has certain quite definite limitations with respect to the conditions which it requires for propagation. The microorganisms responsible for many of the more common and serious of human diseases appear to have no natural breeding place outside of the human body, even though they may propagate in lower animals when inoculated into them; others require the human host for completion of a part of their life cycle. Still others have their essential sources in one or more species of lower animals, though they are able to propagate in the human body also. A few have their permanent sources in the inanimate environment, but these are relatively of little importance.
Diseases due to microorganisms which find their essential source in the human body are capable, so far as this factor is concerned, of a geographic distribution co-extensive with that of man, although this potential distribution may be and frequently is limited by other requirements, which may be obvious as in the case of yellow fever, or still obscure, as in yaws. Those diseases which have their permanent source only in certain species of lower animals are necessarily limited in their geographic range to the distribution of these animals; and such diseases tend ordinarily to definite geographic limitations and often to irregular distributions. Where the inanimate environment constitutes the only necessary source, the potential distribution of the disease corresponds to the area in which the conditions necessary for maintenance are found. Because of the great mobility of the human individual, diseases of solely human origin have, in this circumstance, the potentiality of spreading more rapidly than those propagated in a less mobile reservoir of lower animals; but in fact the rapidity of spread of epidemic diseases seems to be largely determined by factors other than mere rate of travel, though this is a limiting condition.
Vehicles and Conditions of Transmission.—The conditions which have the most obvious influence in determining the distribution of an infectious disease' are those relating to the avenues by which the microorganism escapes from its reservoir, its portals of entry for establishment in a new host, and the conditions necessary for its conveyance from an existing source to this portal of entry. The most common avenues of escape from the living host are through the excretions from the respiratory tract, the alimentary canal, the genito-urinary tract, or the conjunctiva, or from open lesions on the external surface of the body; and, in general, the microorganisms which escape thus have a corresponding portal of entry, those escaping in respiratory excretions becoming implanted on the respiratory mucous membrane, etc., though there are many exceptions to this rule. Also, in general, this group of microorganisms requires only mechanical conveyance from its source to a new host, and usually these organisms are capable of only a brief existence outside of the living host under natural conditions, although to this again there are notable exceptions, such as the tubercle bacillus. Another important group of microorganisms escapes through the agency of blood-sucking insects, which thus become the vectors of infection, either injecting the microorganisms directly into new hosts, or depositing them upon the skin, whence they may subsequently gain entrance, as seems to be the usual mode in the transmission of plague by fleas. In certain of the insect-borne diseases, such as yellow fever and malaria, the insect vector may be an obligate host, necessary for one phase of the microorganism's life cycle; and in such cases the potentiality of conveyance is apt to be limited to a single genus of insects. In other diseases, the insect may act as a mechanical conveyor, in which the organism may or may not multiply; and in some of the diseases thus conveyed other modes of infection may be potential and even, as in tularemia, of considerable relative importance. The life of the microorganism in the insect may be limited by the life of the originally infected insect or may be continued in successive generations of progeny infected from the parent.
In general, the simpler the conditions of transmission the wider is the potential distribution of the disease; hence, diseases transmitted directly from person to person by the respiratory secretions are capable, so far as transmission is concerned, of world-wide distribution, and, if their distribution were limited only by the chances of exposure, would be practically universal. Measles may be cited as a disease which has such a distribution and which, except in very isolated regions, appears actually to attack almost every individual before adult age is reached. Other diseases, such as scarlet fever and diphtheria, though apparently requiring only the simplest of conditions for transmission, attain less general prevalence and more irregular distribution, at least as clinically distinct diseases.
Diseases which are transmitted directly from man to man by mechanical transference of excreta from the digestive tract tend generally to a geographic distribution which is hardly if at all less extensive than that of the respiratory infections.1 They are, however, apt to be of a less regular distribution, since the opportunities for exposure to infection conveyed in this way vary widely in different communities. Also it appears that some of these diseases, as, for instance, bacillary dysentery, are greatly limited in their prevalence by factors other than those which have to do with exposure to the specific microorganism.
1 To this there are striking exceptions, notably the geographic limitations of cholera as an endemic disease.
Diseases which are necessarily or usually transmitted either from man or from lower animals by insects, acting either as biological hosts or as mechanical vectors, are largely governed in their geographical, social, and seasonal distribution by the distribution and habits of insect vectors; and in this class of diseases strikingly limited geographical distributions are often found, as in yellow fever and malaria.
Characteristics and Habits of the Population.—It is evident that in any population the chances of exposure to any given specific microorganism are dependent not only upon the character of the sources and the conditions of transmission of the microorganism, but also upon the characteristics and customs of the population as a whole and of its component groups. For instance, the opportunities for direct transference of respiratory infection must be generally proportionate to the range and frequency of intercourse; the opportunities for exposure to digestive tract infections would depend largely upon proximity of dwellings, customs with respect to excreta disposal, and character of food and source of drinking water; other things being equal, exposure to infection by lice will be proportionate to intensity of intermingling and habits of personal cleanliness, etc. In fact, there is hardly an individual or community custom that has not some obvious relation to the chance of exposure to some specific infection, hence it is useless to multiply examples.
Character of the Reaction Between the Microorganism and Man. —If the epidemiological characteristics of infectious diseases were shaped wholly by the conditions which determine the chances of man's exposure to different specific microorganisms, it would perhaps be possible to analyze quite fully the characteristic distributions of diseases which would result, or even to deduce them, since for many diseases the specific microorganisms, their sustaining reservoirs, and the essential conditions requisite for transmission are known. However, it is necessary to take into account another set of factors concerning which present knowledge is much less definite, namely, those which determine the outcome of the reaction between the microorganism and the human host after effective contact has been established.
The introduction of a specific microorganism through its natural portal of entry into the body may be followed by any one of several results, namely:
(1) The microorganism may fail to secure lodgment, being swept away in secretions or destroyed by the nonspecific outer defenses of the body, producing no effect upon the host.
(2) The microorganism may effect lodgment and multiply, but may establish only a saprophytic relation to the host, who becomes a so-called "passive carrier" of the germ. The pathology of this condition is not fully understood. If the role of the host is in fact purely passive, with no specific reaction whatsoever, the condition should probably be called one of infestation rather than infection, reserving the latter term to apply as defined below.
(3) True infection may result; that is, the microorganism may become established in the body and multiply, eliciting, on the part of the host, a reaction which is specific for that microorganism, not merely a reaction involving the non-specific defenses of the body. This reaction, requiring a more or. less variable incubation period for its full development, may be either clinically characteristic or so ill-defined as to escape clinical recognition; its course may extend over a few days, as in measles, or over years, as in certain forms of tuberculosis; it may terminate eventually in death, in recovery with complete elimination of the microorganism, or in clinical recovery but with continued propagation and discharge of the specific germs. Where recovery occurs, the host may have acquired some degree of specific immunity of a high or low order, durable or transient, and apparently either local or general. It is possible also that certain specific infections may confer some degree of nonspecific immunity against other infections.
From the epidemiological and clinical point of view a distinction may be made between "infection" and "disease", defining disease as an infection accompanied by a reaction clinically distinguishable at the time, while infection without the disease1 or " subclinical infection" is defined as a reaction without clinically distinguishable symptoms. The distinction is perhaps arbitrary and at best relative, since an advance in diagnostic science may transfer cases from the class of subclinical infection to the class of disease; also, in many diseases, the only cases of infection which can be identified at all are those accompanied by distinctive clinical manifestations, so that in these diseases sub-clinical infections may be somewhat hypothetical. The distinction is useful, however, in some diseases, certainly in tuberculosis, where postmortem examinations and specific immunity tests alike give evidence of the past occurrence of true infection with no history of any reaction that could properly be called clinical tuberculosis.
1 Cases actually undiagnosed but which might have been-identified with some degree of certainty by skillful clinical study, would be considered, according to this classification, as cases of the disease, "missed" because of inadequate diagnosis.
In any given case the outcome of inoculation may be a matter of chance in the mathematical sense, that is, it may be the result of a combination of circumstances so complex as to be beyond analysis, and which might not tend, constantly or usually, to bring about this result rather than some other. For example, it may be a mere matter of chance whether a few typhoid bacilli, taken into the alimentary canal, will be swept through or destroyed or will find favorable lodgment. Nevertheless, different diseases tend so definitely to characteristically different frequencies of the several possible events as to leave no doubt that these are determined by specific biological characteristics of the microorganisms and of the populations upon which they react.
The qualities of a microorganism which determine the outcome of the reaction may be defined as: its infectivity 1 considering this as the measure of the microorganism's ability to adapt itself to the environment of the human body to the extent of finding lodgment and multiplying; its pathogenicity, which is defined as the measure of ability, when lodged in the body, to set up a specific clinical reaction, either general or local; its virulence, which is regarded as a measure of the severity rather than the constancy of the clinical reaction; and its "antigenic power," or ability to cause specific immunity in the host.
1 The terms "infectivity," "pathogenicity," and '' virulence'' are commonly used more or less indiscriminately. To avoid confusion, infectivity and pathogenicity are denned as above for the purpose of this discussion, and "virulence" is considered to refer to the clinical severity of infection.
These terms are used as descriptive of properties of the microorganism which may be defined, and in which the variations need not necessarily be parallel, rather than as objective characteristics which are separately measurable. The quite different reactions which different specific microorganisms produce in the same population is evidence that the qualities which have been enumerated are combined in different proportions in different species of microorganisms and apparently in different strains of the same species, though as to this the evidence is usually more complex.
On the part of the human host, the factors which determine the outcome of specific inoculation may be summed up in the general term susceptibility or its antithesis, resistance, which may be resistance either to lodgment and growth or to pathogenic effects after lodgment has been established, thus comprising the whole mechanism of specific and nonspecific natural defenses against infection. In addition to readily demonstrable differences with respect to acquired specific immunity, there is good evidence of variations in racial susceptibility to various infections. There is also evidence that individuals of the same racial stock and specific history vary in their net resistance to specific infections, and there is experimental evidence, as in active immunization against diphtheria, that individuals show quantitative variations in their response to the same antigen.
These characteristics, both in specific microorganisms and in man, may be considered relative rather than absolute, subject potentially to all degrees of quantitative variation, not only as between different kinds of microorganisms and different broad groups of population, but as between strains of the same organism and individuals of the same general group. Since these factors are at present so nearly indeterminate in a quantitative way, it is clearly impossible to demonstrate in detail just how their variations operate in governing the distribution of any single disease; but, granting the existence of such variables, it is possible to distinguish at least the kind of effect which certain combinations of characteristics would have, and to cite examples of diseases showing distributions of corresponding general character.
For instance, it follows from the definition given above that a specific microorganism of high infectivity and high pathogenicity would tend, by reason of its high infectivity, to cause infection in a large proportion of those exposed; and because of its high pathogenicity, the number of clinical cases would approximate the number of persons actually infected. A specific microorganism possessing these qualities in high degree, and directly transmissible from man to man by simple contact would sweep through a population not specifically immunized, affecting a relatively large proportion, as has been observed in epidemics of measles and smallpox in populations which had remained free from infection for many years. Since the majority of the individuals infected under this assumption would give evidence of their infection by a clinical reaction, it should be possible under favorable circumstances to trace rather fully the lines of contact between successive cases; and this again is notably true of smallpox and measles in rural communities. If the specific microorganism had also high antigenic powers, causing a firm and durable immunity this would ultimately become the principal factor in limiting prevalence of the disease. This is obviously the case at present with measles, which is known to confer a strong and lasting immunity, since ninety per cent or more of adults in a country where communication is active give a definite history of having suffered clinically recognizable attacks of measles. In the absence of chronic germ carriers, such a disease, if due to an obligate human parasite, would die out in any but a large population. This likewise is true of measles in small, isolated populations. Yellow fever may be cited as another disease possessing, perhaps, as high infectivity as measles, and equally high immunizing properties, and perhaps also equal pathogenicity though characteristically producing less distinct clinical reaction in children and in negroes. The principle of its spontaneous elimination in small populations by immunization of the human host, even in the presence of abundant mosquitoes for its conveyance, has been beautifully presented by Carter, and has been applied with brilliant success in eradication of the disease.
A high infectivity and pathogenicity, combined with low immunizing properties, would result in a distribution of the disease which would be nearly coextensive with exposure to the specific microorganism; and if this exposure were frequent and widespread the result would be almost universal recurrent attacks. If the minor respiratory diseases which are commonly grouped together as '' colds'' may be considered as caused by a single specific microorganism—a proposition which is by no means established —the infective agent must be considered as possessing this combination of high infectivity with low immunizing properties. A similar inference seems warranted with respect to epidemic influenza ; and the virus of herpes must also, on similar evidence, be considered to confer only temporary immunity or to include a considerable group of immunologically distinct strains.
A specific organism of high infectivity but low pathogenicity would tend to a quite different distribution of clinical cases. Of the persons effectively exposed, many would become passive germ carriers or develop mild clinical reactions not pointing to a specific diagnosis; but the incidence of clinical cases would be small, being limited not by the high infectivity but by the low pathogenicity of the microorganism. Even if the infection were communicated from person to person by direct contact, the lines of contact would, under these conditions, be difficult to trace, since a large proportion of the active sources of infection would be passive carriers not recognizable as such by clinical observation. The meningococcus affords an example of a microorganism possessing this combination of high infectivity and low pathogenicity, since the incidence of carrier infection is demonstrably much higher than that of clinical meningitis. The diphtheria bacillus is another organism demonstrably possessing low pathogenicity in proportion to its infectivity, since the bacteriologieally demonstrable carriers greatly exceed the clinical cases. In this disease the Schick test affords evidence that the occurrence of the disease is limited by a very general specific immunity, which is so distributed in different populations as to warrant the inference that it has been acquired as the result of subclinical infection, which, in turn, indicates considerable antigenic properties on the part of the microorganism. Also, the past history of diphtheria and its present geographic distribution and clinical types, when interpreted in connection with observations on the distribution of the bacillus and of demonstrable specific immunity, afford strong evidence of variations in the pathogenicity and virulence of this microorganism, which apparently have not been parallel to variations in infectivity and antigenic properties.
A low degree of infectivity in a microorganism would imply a correspondingly low rate of actual infection; and, given an infectivity so low that infection would result only from massive, prolonged or repeated exposure, the prevalence of the resultant disease could be sustained only by long continued chronic infection of the human host, or by some sustaining reservoir other than the human body. If the epidemiology of leprosy is correctly interpreted, the lepra bacillus may serve as an example of a microorganism possessing such low infectivity that its continued existence, if it be an obligate human parasite, is dependent upon long continued infection of the individual. The foot-and-mouth disease of cattle may be cited as one of such low infectivity for man that it could not be sustained as a human infection without a reservoir in lower animals.
These few examples are cited merely to illustrate the general principle that the factors which govern the reaction following potentially effective contact between specific infective organisms and man may bring about a distribution of the disease which is quite different from the distribution of exposure, or even of infection. It is evident, however, that the two sets of factors, those governing exposure and those governing the occurrence of infection and disease following exposure, are intimately related in various complex ways. Thus, the nature of the host's reaction to a microorganism, determining whether the infection be chronic or of short duration, is intimately related to the chance for exposure of other individuals; and the same may be said of such immunization as prevents the individual from being later a source of exposure for other persons. Also, it is evident that the factors which have been stated chiefly in terms of the properties of specific microorganisms might have been stated equally well in terms of the complementary characteristics of their hosts.
The Broader Distributions of Infectious Diseases.—It is convenient, for purposes of discussion, to distinguish such broad distributions of diseases as are shown by a view covering relatively large populations and extending over considerable periods of time, from their more local distributions within each population in relation to details of environment, personal habit, past history, and individual constitution. While the epidemiological characteristics of a disease cannot be separated in fact in any such way, the distinction has the justification that the data required for description of the broad and the detailed features, respectively, are not only of quite different scope, but usually come from different sources.
The features, of each disease which are classed here as its broad, general epidemiological characteristics, are such distributions as may be described from data which are simple in character but of wide extent. Even these broad features are so varied in different diseases and, indeed, so complex in any single disease, that no single plan of classification and presentation is of general application. A broad epidemiological description of a disease should include, however, as a minimum, a statement of the area of known occurrence of the disease, its observed gross rates of prevalence in different populations in.successive periods of time, and its relative frequency of occurrence in different racial, sex, and age groups. These statements may then be related to broad differences in the composition, history, and environment of the different populations referred to.
Data Required for Description.— For the quantitative description of such broad epidemiological features, it is necessary, in the first place, to have adequate statistics of population in each area, in sufficient detail to permit separation of distinct racial, sex, and age groups. Then, in order to make up similar summaries of the cases of the disease. classified according to the successive time periods in which they have occurred, it is necessary to have, for each case, a record of its date of occurrence, and of the location, race, sex, and age of the person affected. Simple as are these data, they require, for their systematic collection, fairly elaborate enumerations or estimates of population; a medical service adequate to insure observation and correct diagnosis of the disease as it occurs; and a well-developed system of morbidity reporting.
At present the basic statistics of population are lacking for very many large and populous areas, and it is only in limited areas that the other essential requirements as to diagnosis and reporting of cases are fulfilled even for the more distinct and serious of infectious diseases. Moreover, where these conditions are fulfilled, this has been accomplished only in comparatively recent years. Therefore, it is not yet possible to give a quantitative picture of the world distribution of any single disease over any considerable period of time. Nevertheless, it is possible to select from fragmentary records data sufficient to give a fairly clear and distinctly significant picture of the broader distributions of the more important diseases. Data which are not exact in a quantitative sense may still serve to show the area of occurrence of a disease; to indicate, if not to measure, epidemic and seasonal f actuations; and to give an approximate idea of distinctive age-distributions. For many purposes mortality statistics may be used as an index of morbidity; and for more accurate quantitative comparisons, more exact morbidity statistics from sample areas may serve. It is possible, therefore, to develop distinctive, if not exact, epidemiological descriptions of many diseases from data which might appear to be hopelessly imperfect. Moreover, even if the necessary data were available, the full statistical description of the broad epidemiology of a single wide-spread disease would be a large undertaking, and, though valuable as a work of reference, such a compilation would probably be less generally informative than the usual kind of discursive account based on selected material.
Interpretation of Broad Epidemiological Characteristics.—The significance of the broader epidemiological distributions which are found to be characteristic of any disease lies principally in the light which they may throw upon the more general limiting conditions of occurrence. In this application the broad features may widely extend knowledge of the general factors which govern the occurrence of a disease like diphtheria, concerning which the experimental data are relatively full; or they may point to quite definite and legitimate inferences concerning essential sources and routes of infection in diseases such as lethargic encephalitis or influenza, where the experimental evidence is not yet definitive. In any interpretation it is, of course, requisite that the various features of distribution be considered in their combinations rather than separately, and that they be put together with such facts as are known from more detailed local studies and from experimental investigations. Hence, the full significance of broad epidemiological characteristics can be illustrated adequately only by extended analysis of the epidemiology of individual diseases, which is beyond the scope of the present discussion; but a few fragmentary examples may serve to illustrate the kind if not the extent of the general inferences which may be drawn.
Area of Occurrence.—A knowledge of the area within which a disease has occurred may have a definite significance in relation to the nature of the sources and routes of infection which are essential to its transmission, since the disease will not be more widespread than the necessary sources and vectors of the specific organism. Thus, the bare fact that a disease is known to have occurred and spread in all parts of the world makes it certain that the climate, fauna, or other environment which are peculiar to any less limited area cannot be essential factors in its transmission. Conversely, the fact that a disease occurs only within well defined geographic limits may constitute presumptive evidence that some environmental condition peculiar to these areas is necessary to its propagation, and may point to the direction of significant experimental investigation, as was the case in the history of malaria and yellow fever.
Regularity of Geographic Distribution.—The distribution of a disease in various geographic subdivisions within the area of occurrence may also be significant of the general conditions requisite for transmission. A fairly uniform distribution, not consistently related to such conditions as climate, density of population, and habits of life, indicates that the conditions of transmission are simple, as, for example, in some of the acute exanthemata and in influenza. An irregular distribution, characteristically high in certain localities and low in others, suggests, on the contrary, that either the sources of infection or the conditions of transmission and infection are not uniformly distributed; and the kind of environment associated with the higher prevalence may suggest the nature of the special conditions which are concerned.
Limiting Rate of Prevalence.—The characteristic or limiting rate of prevalence which is established within the area of known occurrence may likewise suggest sources and modes of transmission to be considered. Such a high rate of observed prevalence as is characteristic of measles or of smallpox in unvaccinated populations is quite consistent with the hypothesis that the observed clinical cases may be the chief, if not the sole, sources of infection. On the other hand, a sporadic distribution of cases widely separated from -each other, as in the endemic occurrence of poliomyelitis, indicates the existence of a concealed reservoir of infection, suggesting as probable sources either passive carriers and clinically unrecognized cases or some of the lower animals.
Seasonal Distribution.— The seasonal fluctuations in rates of prevalence which are characteristic in many diseases can usually be explained, if at all, only in the light of fairly definite knowledge of other associated epidemiological features; hence, considered by themselves, these fluctuations must be interpreted most cautiously. The seasonal distribution may, however, support or negative a particular hypothesis as to the means of spread of a disease of uncertain epidemiology. For instance, the characteristic summer prevalence of poliomyelitis, together with certain other features of its occurrence, suggests that the infection may be transmitted by insects; but the fact that even occasional epidemics occur in severe winter weather excludes a large group of insects from consideration as obligate vectors. Some other considerations regarding fluctuations in prevalence are noted hereafter in the discussion of the phenomena of epidemics.
Age Distribution.—The fact that a particular disease shows a certain generally characteristic age distribution seldom leads, by itself, to any direct inference as to the way in which the disease is spread; but in combination with other facts, a knowledge of the age distribution may materially aid their interpretation. For instance, it has been observed that poliomyelitis, in rural epidemics, is less confined to young children than it is in urban districts, and that the same kind of difference as between rural and urban populations is observed in the age-distributions of other diseases, such as measles, where the difference may be explained as due to the more frequent occurrence of immunizing infection in early life in the residents of cities. In poliomyelitis, since the recognizable disease is relatively rare, if there is any such widespread specific immunization it must be due to sub-clinical infections, which have not been directly demonstrated. Still, this characteristic variation in age-distribution, when taken in connection with a series of other facts, tends to support the view that poliomyelitis actually is quite prevalent as a sub-clinical infection.
Epidemics.—The course of an infectious disease in a large population seldom if ever shows a consistently sustained rate of prevalence. The mean rates of incidence in successive periods of years or decades may not vary much, or, if they vary, may follow a fairly simple trend; but in shorter periods of weeks or months the rates usually oscillate more or less widely around this trend line as an axis, in alternating periods of high and low prevalence. In many diseases, such as typhoid fever and diphtheria, these fluctuations are strikingly regular in their range and periodicity ; the peaks of prevalence recur annually at about the same season; and the range of the excursion from maximum to minimum is of about the same magnitude from year to year, or perhaps tends to diminish regularly and progressively. In other diseases, of which measles and scarlet fever are good examples, the fluctuations are less regular. Each year may show a more or less distinct peak of prevalence, falling usually within a certain seasonal range; but in successive years the fluctuations are of quite uneven range, and at intervals of several years major peaks occur, quite out of the range of those which mark the intervening years.
In common usage these peaks of incidence are called "epidemics" only if they are somewhat unusual in range or in some circumstance which links them together as attributable to a common cause. Thus, it is usual to refer to a dozen cases of typhoid fever among the guests at a single dinner as an epidemic, though the incidence rate in the community as a whole may not be materially increased by this small number of cases. Again, the major waves of measles, which recur every few years, are called epidemics; but this term is not usually applied to the annual seasonal increase in occurrence of diphtheria. As the distinctions which are thus made are somewhat vague and are not altogether consistent, it seems preferable and allowable, for purposes of general discussion, to define an epidemic more broadly, as any temporary increase in the prevalence of an infectious disease of such extent and course as to indicate a definite change in the balance of forces controlling the occurrence of the disease in the population. Where the entire course of the disease is made up of oscillations, this definition would describe them as a continuous series of epidemics, the period of each epidemic extending from the point which marks the beginning of an upward trend to the point which marks the lowest level in the subsequent decline.
In any case, whether an epidemic be of -usual or unusual range, and whether it be due to rare or to regularly recurrent circumstances, it represents essentially a definite phase in the equilibrium of a reaction in which three factors are concerned, namely; a specific microorganism, a population, and the particular set of environmental conditions which govern the rate of potentially effective contact between these two. The causes of epidemics are, therefore, determinable in proportion as the variables concerned in this reaction may be analyzed; and while this may be done with fair precision in certain instances, it is a matter of extreme complexity in others, for each of the three factors mentioned above may comprise in itself a complex group of variables which may be diversely related to each other, and which are wholly or partially indeterminate by such observations as are practicable. The complexity of these variables and the difficulties in the way of measuring them may be illustrated by noting some of the more obvious variations. In this discussion it will be assumed that the specific microorganism' concerned is an obligate parasite, either of man or of some lower animal which is associated with the human population, since the known exceptions to this condition are relatively few and unimportant in human epidemiology.
The microorganism may vary in numbers, of which an index, though not necessarily an accurate measure, is afforded by the number of infected individuals in the- population, including indistinct cases and "carriers," which may be extremely difficult or impossible of detection and enumeration. It may also vary in specific properties, notably in infectivity and pathogenicity. The measure of infectivity is the frequency of infection resulting from inoculation of a given number of microorganisms into groups of hosts of the same susceptibility ; but this measure can be applied directly only under experimental conditions, and even then with difficulty. The index of pathogenicity is the ratio of clinical to sub-clinical reactions resulting from infection. This is determinable where means are available for recognition of sub-clinical and passive infections, as in diphtheria and cerebrospinal meningitis, but even in such cases the observations actually made are seldom sufficiently exact or extensive to measure the variations which may take place.
On the side of the population, the variable which is difficult to determine is susceptibility. With respect to certain diseases, such as measles, smallpox and yellow fever, there is good evidence that susceptibility to infection is approximately coextensive with susceptibility to the disease, and that, except in those who have been specifically immunized, susceptibility is relatively high and well nigh universal, so that the mass-susceptibility of the population is determined by the ratio between two sharply differentiated groups, one made up of individuals who are highly susceptible and the other of those who are highly resistant as the result of previous specific immunization. By careful observation both of these groups may be enumerated with some approximation to accuracy, affording an index of mass-resistance. There is equally good evidence that in other diseases mass-susceptibility varies in a more complex way so that it must be represented by a more elaborate frequency distribution, in which many grades of individual susceptibility are represented; and in some diseases variations in susceptibility may be partially independent of prior contact with the specific infective agent. Also, susceptibility to a specific infection may be far more frequent than susceptibility to the disease, as is demonstrably the case in diphtheria and tuberculosis. The measure of susceptibility is the frequency and character of the reaction to a given dosage of a specific microorganism of constant properties, and can be applied only in controlled experiments.
The rate of exposure or potentially effective contact between the specific microorganism and the host population is never directly determinable except under experimental conditions, and variations in the rate in any natural population can only be inferred from other observations. These may be of such kind as to clearly indicate a change in opportunities for conveyance. For instance, an observed increase in prevalence of anopheline mosquitoes would quite definitely imply increased opportunities for the conveyance of malaria; but even in such cases it may be impossible to ascertain just how much the rate of effective contact is affected, since the actual dosage of microorganisms inoculated is always indeterminate in natural conditions. Moreover, very little is known, in a quantitative way, of the relation which increase of dosage or repetitions of exposure bear to the probability of infection.
If the several variables which have been mentioned were entirely independent of each other, the whole course of an epidemic might be determined by the changes in a single factor, all the others remaining constant; but in this case the variation in the single factor must be temporary in its effect or must be reversed, operating first to increase and then to diminish prevalence of the disease, since an epidemic implies not only a rise but a subsequent decline in morbidity. It is not likely that the variables are ever entirely independent of each other in nature, but special cases may be cited in which it is probable that the course of an epidemic is governed principally by variation in one factor alone.
For example, it seems fairly certain that the incidence of typhoid fever in most of the large cities of this country is held down to its present low level chiefly by environmental conditions which restrict the opportunities for transfer of the typhoid bacillus from person to person, rather than by resistance of the population or enfeeblement of the specific microorganism. Therefore, any circumstance which temporarily increases the rate of transference of the typhoid bacillus from existing sources to the surrounding population may, by itself, give rise to an epidemic. This is essentially what happens when a water supply or a milk supply which is distributed to a considerable number of people is accidentally contaminated with typhoid bacilli. If the infections are not sufficiently numerous to materially reduce the mass-susceptibility of the population, and if the secondary eases resulting from the primary increase in number of foci of infection are relatively few, the whole course of such an epidemic may be governed by the extent and duration of the increased exposure brought about by contamination of the common medium. In the simplest case, where the mass exposure is limited to a single day, the distribution in time of the onsets of primary cases will represent merely the distribution of incubation periods.
There are other instances in which variation in some other single factor might be concerned. For example, it is well known that the number of persons; harboring pneumococci greatly exceeds the number suffering from pneumonia, hence that the occurrence of this disease is limited not by the rarity of exposure to the specific microorganism, but rather by host resistance or by low pathogenieity of the pneumococcus. Therefore an epidemic of pneumonia might result either from an increase in the pathogenic properties of the pneumococcus or, independently of this, from a lowering of mass-resistance, as for instance by an epidemic of measles or influenza.
The above examples are cited merely to illustrate the possibility that variation in a single factor may govern the course of an epidemic. These, however, are special cases, for it is certain that the variables concerned in the equilibrium of infectious diseases are not really independent, but are intimately related to each other. Although these relations differ in different diseases, there are two which are quite general. One is the relation between the number of infected individuals in a given community and the exposure of the rest of the population. Thus, assuming that the . number of exposures in the population bears a constant ratio to the number of infected individuals present, any increase in. the number of the latter, no matter what its primary cause, tends to increase the total exposures in the community, and, other conditions being equal, this causes a further increase in the number of infections in a later time interval. In the absence of some counter-balancing force this increase in the number infected in successive time-intervals would continue in a geometric progression until the entire population had been infected. The other general relation, which tends automatically to check such progressive increase in rate of prevalence, results from the fact that infection usually, perhaps invariably, confers specific immunity of some degree upon the individual host, so that as the number of infected individuals in a population is increased the number of susceptibles available for infection in succeeding time-periods is correspondingly diminished. Where infection results in death of the host this also quite obviously diminishes the supply of susceptibles for subsequent infection.
If all other factors remained constant, the interplay between these two opposing but mutually dependent forces, one tending to progressively increase the prevalence of infection and the other to progressively diminish it, would eventually establish a stable equilibrium, in which the number of new infections occurring in any given time period would be exactly equal to the number of susceptibles added by births, immigration and lapse of immunity. It is probable, however, that in nature other factors never remain constant for any considerable period; and a comparatively slight change in any one of them may set up a fairly wide oscillation in the rate of prevalence. For instance, a seasonal change in weather might tend to increase the rate of exposure, due to a change in habits of the population, or perhaps might operate, either directly or indirectly, to lower resistance to infection, thus starting an upward swing in the rate of prevalence. The resultant primary increase would then tend to establish a further progressive increase because of the increased number of sources from which to spread; and this, in turn, would result in a compensatory mass-immunization, which would not only check the increase, but would eventually depress the rate of infection below the level of equilibrium, thus preparing the way for a subsequent upward swing by way of readjustment. Probably a general explanation of epidemics is to be found in some such sequence of events as this, oscillations above and below the axis of equilibrium being kept up by occasional and perhaps slight changes in any one or more of the variables which enter into the reaction.
In attempting to apply this general explanation to the observed phenomena of particular epidemics, two principal questions arise, namely: (1) as to what factor has been responsible for the primary impulse toward an increase in the prevalence of infection; and (2) as to whether mass-immunization is generally sufficient, in itself, to bring about the decline of an epidemic. Referring first to the latter question, it needs lo be borne in mind that to check an epidemic and bring the rate of prevalence temporarily below the level of equilibrium it is by no means necessary that all the susceptibles in the population must have been infected. They need only be reduced below a certain critical ratio, which varies in accordance with other conditions. Then too, a considerable proportion of individuals, even though not specifically immunized, may have a natural immunity to certain infections, so that those initially susceptible may constitute only a fraction of the total population. Also, what is of great importance, the prevalence of immunizing infection in an epidemic may be much greater than is shown by the incidence of clinically recognizable cases of the disease. Of such immunization by sub-clinical infection there is direct evidence in epidemics of diphtheria and quite convincing though somewhat indirect evidence in epidemics of poliomyelitis. Experimental studies of epidemic infections in mice by Webster and by Topley and his associates have also given evidence to the same effect. Therefore, the effect of an epidemic, as regards mass-immunization, may be far greater than would appear from the observed ratio of morbidity to population.
As to the particular variable that is responsible for the initial impulse of an epidemic, there is no presumption that it need be the same in all epidemics. In certain annually recurrent seasonal epidemics, there is good reason to believe that the first influence is an increase in the rate of transfer of the specific agent from infected individuals to others. This seems to afford an adequate explanation of the inception of seasonal epidemics of certain insect-borne diseases such as malaria, yellow fever and plague (in rats); and to give a possible and partial explanation of the characteristic seasonal increase in some other more directly transmissible diseases, such as diphtheria and pneumonia. However, no such obvious explanation applies generally to the origin of the occasional wide-spreading epidemics which occur in the history of influenza, poliomyelitis, cerebrospinal meningitis, lethargic encephalitis, and many other typically epidemic diseases. It is seldom that the origin of these epidemics is associated with any determinable increase in such intercourse as would tend to increase the rate of spread from person to person, or with any objective change in environmental conditions which might be supposed to suddenly and greatly influence mass-resistance. In the light of present knowledge the most generally acceptable explanation of an epidemic of this kind is that it owes its origin to a change in the properties of the specific infective agent, which somehow acquires greater infectivity, greater pathogenicity or both. As regards the experimental evidence in support of this view, it is demonstrable that many microorganisms vary in their infective properties under experimental conditions; but it has not been clearly established that such changes are characteristically associated with epidemics. The evidence from experience is of a kind which cannot be presented adequately except in connection with a detailed analysis of the whole epidemiology of each disease; but when so presented it is quite impressive with respect to each of the diseases mentioned above and for a number of others. This is especially the case where a change in the clinical type of a disease is associated with an epidemic, and where the level of prevalence remains for a long period higher than it was before the epidemic, as illustrated in the history of diphtheria during the last half of the nineteenth century, and the more recent history of poliomyelitis.
Laws of Epidemics.—There appear, then, to be two general laws of epidemics; first, that infection tends to increase progressively, due to multiplication of foci; and second, that it is progressively cheeked by the resultant decrease in susceptibles, due to specific immunizations and deaths in the host population. The known differences between different diseases as regards variability of the specific microorganism, its period of survival in the individual host, the ratio of sub-clinical to clinical infections, the character and distribution of natural host resistance, the degree and durability of acquired immunity, and the kind of conditions necessary for conveyance from host to host—all these are sufficient to account for the widest differences in the periodicity and range of epidemics in different diseases. Presumably the balance between the many variables is not the same in any two diseases, and there is no presumption that an exact quantitative analysis of the interplay of factors which govern in epidemics of any one disease would be fully and directly applicable to any other infection.
THE DETAILED DISTRIBUTION OF DISEASES, WITH SPECIAL REFERENCE TO THEIR INVESTIGATION AND INTERPRETATION
Sufficient examples have already been cited to illustrate the general statement that every disease has a distribution peculiar to itself, in that its occurrence is associated with certain peculiar conditions of environment and of special circumstance in personal history, habits, and characteristics. These associations may be in part deduced from facts established by direct observation of the specific microorganism if this has been isolated and identified, or by certain crucial experiments with material containing the specific virus even without its actual isolation. There remain, however, many characteristic features in the distribution of any disease which can be ascertained only by studying the circumstances under which the disease occurs in nature, sometimes by broad observations and sometimes by intensive local investigations which must go into rather minute detail. The character, collection, and significance of the data which describe an infectious disease in terms of its detailed distribution can be discussed only by presenting a few illustrative examples.
General Significance of Combined Epidemiological Characteristics.—The association of a disease with any particular condition or set of conditions may be such that the disease never occurs except in the presence of this condition, which is thus established as a necessary or limiting condition for the occurrence of this disease; or it may be that the association is less complete, so that the disease occurs more frequently where the condition exists, but sometimes without it. The distribution of yellow fever affords a ready example of such associations with special conditions, some of which are necessary, and some favorable, but not necessary for its occurrence. Thus, it has long been known that a limiting condition for the sustained endemic prevalence of this disease was a climate such as is found only in definitely circumscribed geographic areas; that outside of these endemic zones, the disease sometimes occurred and spread in other broader areas, but subject there only to further limiting conditions of season and temperature, and of recent communication with some previously infected place. On closer study of populations in which the disease prevailed, it was found to occur very seldom in people who had suffered a previous attack, or who had spent their childhood in an area of endemic prevalence. In epidemics, the occurrence of yellow fever was known to be associated with the houses in which cases had previously occurred; but this was recognized as not being a limiting condition, since cases occurred also in those who had not entered infected houses.
It was a long series of observations of this kind, showing certain conditions which limited and others which favored the occurrence of the disease that led up from one side to the formulation, testing, and experimental proof of the hypothesis that yellow fever was conveyed from man to man by the bite of a particular species of mosquito. Again, after it had been proved that yellow fever was thus conveyed under experimental conditions, it was the facts known about the natural distribution of the disease which confirmed the theory that this was probably the only means of conveyance in nature. In more recent years, with this theory firmly established, it has still been necessary, especially in connection with preventive measures, to make detailed studies of the occurrence and spread of yellow fever in a number of different areas; but any such study may now be limited to investigation of conditions which have a rational relation to the opportunities for conveyance of the infection from man to man by the known mosquito vector.
The special purposes which studies of detailed distributions of a disease in nature may serve in extending knowledge of the epidemiology of a disease, are, in general, those which have been exemplified in the reference to yellow fever, namely:
(1) To indicate the nature, essential sources, and routes of conveyance of the specific infective agent, where these have not been more directly established.
(2) Where the existence of a specific infective agent, its sources and the limiting condition of its conveyance have been experimentally demonstrated, to extend in more detail the corresponding general theory of the epidemiology of the disease.
(3) Where this general theory has already been established, to ascertain, in more detail, the particular local conditions which favor or control the spread of the disease in a given community.
These are not separate and distinct aims, for though one or the other may be most prominent, depending upon the scope of the study undertaken or the stage of development which has been reached in the epidemiology of any particular disease, all three purposes are, to some extent, combined in every study. Thus, the general characteristics in the distribution of any disease are ascertained primarily by local investigations and are established as general features only by accumulation and comparison of local observations. Also, any special set of circumstances found locally associated with the prevalence of a disease must always be interpreted in the way that will be consistent with the more general facts which are already established.
Snow's Interpretation of the Epidemiology of Cholera.—The way in which the broad limiting conditions in the distribution of a disease are fitted in with the details of local distribution, so that each set of observations contributes to the interpretation of the other is excellently illustrated in John Snow's masterly analysis of the epidemiology of cholera. As his methods of collecting, combining, and presenting the data used are unusually simple and direct, his argument will be summarized in substantially the same sequence that is followed in the original.1
1 The sequence as given here is that used by Snow in his most complete exposition, published in 1855. In his earlier presentation of the same thesis, in 1849, substantially the same argument was made, but in a somewhat different sequence and without the support of some of the facts which were available in 1855.
(1) Referring to the fact that cholera, which had been unknown except in India until about 1820, had since then spread widely over the world in a series of epidemics, he observes that it would be of little use to describe in detail how it had caused devastation in some places and passed lightly over others, unless he could at the same time give a full account of "the physical condition of the places and the habits of the people," which he is not prepared to do. He confines himself, then, to stating briefly the limiting conditions of the occurrence of the disease, namely: that the progress of cholera over the world, in its pandemic invasions has been definitely along the routes of commerce, traveling never faster than man travels; "in extending to a fresh island or continent it always appears first at a seaport''; and, though "its exact progress from town to town cannot always be traced,'' it "has never appeared except where there has been ample opportunity for it to be conveyed by human intercourse."
(2) His next statement is that in "innumerable instances," of which some are cited in detail, and hundreds are to be found in the literature of the day, there has been every appearance of the direct transmission of cholera from person to person in definitely traceable series.
(3) The fact that cholera is communicable from person to person is interpreted as implying the transfer of "some material which passes from the sick to the healthy, and which has the property of increasing and multiplying in the systems of the persons it attacks"; and from a previously accepted general principle of biology, it follows that "the morbid matter of cholera, having the property of reproducing its own kind, must necessarily have some sort of structure, most likely that of a cell. It is no objection to this view that the structure of the cholera poison cannot be recognized by the microscope, for the matter of smallpox and of chancre can only be recognized by their effects and not by their physical properties"—a limitation which still exists regarding identification of the virus of smallpox and that of many other diseases.
(4) The pathology of the disease suggests the alimentary canal as the seat of multiplication of the virus, its portal of entry for infection, and its avenue of escape from the body, thus establishing a definite hypothesis as to the mechanism of transmission.
(5) It follows, as deductions from this hypothesis; (i) that infection will be conveyed by food imperceptibly contaminated with minute particles of the cholera dejecta, and that conveyance in this way will be most frequent among those persons who are in close association with cholera patients in the crowded and unclean environment of the poor; (ii) that cholera dejecta thrown into cesspools will contaminate wells, and discharged as sewage will contaminate the water of streams, with the result that municipal water supplies taken from such streams will spread the infection to the more affluent as well as to the poorer classes in the cities; (iii) that a person may (in a clean environment) be in the room with a cholera patient without being "exposed" to the infection; and again, may be exposed without ever having been in close proximity to a person suffering from the disease.
(6) As facts in conformity with the first of these deductions, he cites, as well-known characteristics of cholera, its high prevalence and local extension in the crowded, dirty homes of the poor, its high prevalence in institutions for children and the insane, and its high prevalence in miners, who habitually ate their food in the mines, with no facilities whatsoever for cleanliness; and notes the rarity of secondary eases in the houses of the well-to-do.
(7) As facts in conformity with the deduction of conveyance by water, he describes in detail several intense localized outbreaks of cholera, including the famous Broad Street Pump epidemic,1 in each of which the cases were limited chiefly to persons known to have drunk water from a common source obviously exposed to contamination, and in some instances specifically known to have been contaminated with the dejecta of cholera patients.
1 An excellent abbreviated account of this epidemic in a generally accessible reference, is to be found in Sedgewick's Principles of Sanitary Science and the Public Health, MacMillan, New York, 1902, pp. 170-181.
(8) Continuing the discussion of water as a vehicle, he reviews the history of cholera in a number of British cities in the epidemics of 1832 and 1849, and observes that in those cities which had water supplies of general distribution, taken from sewage polluted streams, cholera extended to all classes of the population, while in the cities with relatively unpolluted water supplies from upland sources or without general supplies, cholera prevailed chiefly in the poorer sections, where it would be spread by transfer from person to person.
(9) Taking up the history of cholera in London, in the epidemics of 1849, 1853, and 1854, he describes the nine separate public water supplies which served the city in 1849, their sources with reference to obvious sewage pollution, and, in a general way, their distribution, noting that the most grossly polluted supplies, furnished by the Southwark and Vauxhall company and the Lambeth company, were two which were taken from the lower Thames and distributed to the districts lying south of that river. He then presents a table showing, for each of the 38 districts of London, the population, the number of deaths and the death-rate from cholera in 1849. Arranging the districts in descending order of mortality rates, he points out that in each one of the nine districts where these two highly polluted water supplies were used the cholera death rate was higher, in 1849, than in any of the other districts of the city. Considered as a group, these districts, with a population of 466,000, had a death rate three times that of the rest of the city. The two water supplies in question were taken from sources about equally contaminated, and the mortality rates in their respective distribution areas did not differ greatly.
(10) By 1853 the intake for the Lambeth supply had been removed upstream beyond the zone of gross sewage pollution, while the Southwark and Vauxhall supply was still taken from the same highly polluted source as in 1849. As compared with all other districts in the city, those which were served chiefly by the Southwark and Vauxhall supply still, as in 1849, showed the highest mortality rates. A table of mortality by sub-districts in 1853, is then presented, showing mortality rates of 11.4 per 10,000 in the areas supplied wholly by the Southwark and Vauxhall Company, 6.0 per 10,000 in the sub-districts served partly by this supply and partly by that of the Lambeth Company, and no deaths in the comparatively small population (14,600) receiving only the Lambeth supply.
(11) By the summer of 1854, when cholera recurred in a quite severe epidemic, Dr. Snow had noted that an area comprising about two-thirds of the population south of the Thames was served by both water companies, the Southwark and Vauxhall, and the Lambeth. As each company had its mains laid throughout this joint distribution area, and as the residents had generally no special preference for one supply rather than the other, some of the houses on the same street took their water from one and some from the other source. By a personal investigation, with some aid from an assistant, Snow ascertained the source of the water actually supplied to each house in which a death from cholera occurred in the south districts of London during the first seven weeks of the epidemic. He then ascertained the total number of houses supplied by each company, and presented the following comparison of mortality:
Thus he showed that in this area one group of the population, using a grossly polluted water supply, suffered a cholera mortality rate nine times that of the other group, consisting of the same kind of people, residing in the same area, living often in adjacent houses, and subject to an environment differing, so far as could be ascertained, only in the circumstance that their usual water supply came from a different and less polluted source. Two years later, after his observations had been confirmed and extended by an official inquiry, he was able to show that this disparity of mortality was consistent in every one of the 23 sub-districts in which the two supplies were mingled.
This abbreviated summary, which gives only the main points in the argument, necessarily omitting much of circumstantial detail, does not show the full weight of the evidence collected by Dr. Snow or the skill with which he forged it into a chain of inductive reasoning which led inexorably not merely to the inference that a specific microorganism was essential in the causation of cholera, but also to the inference of much of the characteristic life history of the microorganism. Even the summary will serve, however, to show the general process of reasoning; how it consists of a series of hypotheses, each leading to quite specific deductions concerning some of the broad and some of the detailed distributions of the disease; how each of these hypotheses is verified by observations confirming the deductions; and how these again lead to still more specific hypotheses, which in turn are verified by further observations; and how every fact shown in the evidence is finally arrayed in a definite order of relation to every other fact.
The Interpretation of Peculiar Local Associations.—The different problems which present themselves in the building up of epidemiological theory are so diverse that it is hardly possible to give any description of the methods which are applicable except to state that they must conform always to the broad principles which govern all similar processes of constructive reasoning. There are, however, several principles of procedure which can be defined rather simply and which are quite generally applicable in one way or another to a wide variety of epidemiological problems especially in local investigations. These may be illustrated by reference to Dr. Snow's analysis; but this can be done more conveniently by proceeding in a direction which is opposite to that followed in his presentation.
Let it be supposed, for the sake of illustration, that Dr. Snow's purpose is not primarily to develop a general theory of the epidemiology of cholera, but that he is concerned for the present only with the specific problem of explaining the distribution of cholera in the south districts of London in the epidemic of 1854. He will then be in precisely the position which a health official or epidemiologist usually occupies to an investigation into the sources and modes of spread of an epidemic or endemic disease in a particular locality.
In order to have a line of attack it is necessary to have, as a starting point, some hypothesis concerning the conditions which are likely to contribute to the prevalence of cholera, but for the present this need be only the very general hypothesis that the occurrence of the disease is in some way associated with the use of sewage polluted drinking water.
The simplest and most direct method of determining whether or not such an association exists, is the method used by Dr. Snow, namely, that of ascertaining what different water supplies are used within the area of investigation, and how those supplies differ with respect to sewage pollution; then classifying (1) the persons who have died from cholera, and (2) the entire population, according to their sources of water supply. It remains to ascertain the frequency of deaths from cholera in each of two groups of the population, which differ with respect to the sources and sewage pollution of their water supplies, that is, to ascertain their ratio of deaths to total persons in each group. If the difference of incidence in the two groups is found, as in this instance, to be entirely outside the range of such differences as may be expected in two groups of such size drawn at random from the population, it may reasonably be inferred that in this area the use of sewage polluted water is positively associated with the liability to death from cholera. It is further found, by still another independent inquiry, that the two groups are, so far as can be ascertained, quite similar in all other conditions of composition and environment, hence the association of cholera mortality with character of water supply is a rather direct one. It is, of course, equally necessary to show that the two water supplies actually differ materially with respect to the degree of sewage pollution.
The association between sewage polluted water and cholera mortality is still further tested and confirmed by examining its consistency in each of the sub-districts included in the whole area, thus making it more certain that the association does not depend upon some unsuspected difference in the local distribution of the two population groups. It is still further tested by extending the observation back to 1'853 and finding that a similar association, which is not demonstrated in such detail, existed in that year. Then, by going back to 1849, when the two water supplies were taken from equally polluted sources, it is found that the disparity of mortality in the sub-districts separately supplied has disappeared. Still further confirmation of the association of cholera with quality of water supplies is afforded by comparison of the south districts with the rest of London; by investigation of several localized epidemics of cholera in other parts of London, in each of which the outbreak was confined chiefly to persons known to have used water from a highly contaminated local source; and by considerable detail not reproduced in the summary which has been given here. Finally, extending the inquiry to other British cities, evidence of a more general character is found indicative of a similar association there between pollution of the water supplies and the mortality from cholera.
In the meantime, it has been found that although cholera mortality is intimately and quite generally associated with the use of sewage polluted drinking water, this is not a necessary or limiting condition in the occurrence of cholera; and that in certain districts, the prevalence of the disease is associated with an unclean domestic environment and with proximity to a previously affected person. This association is also found to be not peculiar to London, but quite characteristic of cholera in many localities. It may be mentioned here that the association of cholera with filth is not actually demonstrated in a statistical way. It is stated rather as an association which is obvious and has been generally noted by all observers.
Referring back to the water supply, it has now been established very definitely, by a series of processes which are essentially statistical, that there is a real and quite general association between cholera mortality and the drinking of sewage polluted water; but this fact by itself tells nothing of the mechanism by which polluted water contributes to mortality. If it be assumed, as a hypothesis, that cholera is an infectious disease, then it can be deduced that any condition positively associated with the occurrence of the disease must operate either to increase exposure or to increase susceptibility, or in both ways. On purely a priori grounds one explanation is as probable, as the other; and, in fact, most of Snow's contemporaries, recognizing the association, concluded that polluted drinking water increased individual susceptibility to the influence of a cholera poison which was generally diffused in the atmosphere. In order to demonstrate that drinking polluted water tended to increase the exposure rather than the susceptibility to cholera, it was necessary for Dr. Snow to show that this was the only view of the relation which fitted into a general and comprehensive theory of the epidemiology of cholera. In other words, before the association of polluted water with cholera could be "explained," it must be related to the association of cholera with filth, and to every other fact known about the local and general distribution of the disease; and must then be related, through these facts, to the epidemiology of communicable diseases in general, in a theory which eventually leads back of this to the peculiar properties of the virus of smallpox, and from this again to the broad principle of biogenesis as applied to microscopic organisms.
Some General Principles of Procedure.—The principles of epidemiological procedure which the analysis given above is intended to illustrate are quite general. They are:
(1) In every epidemiological investigation, whether its immediate purpose be to explain a localized epidemic or to elucidate the general spread of an obscure disease, the first step is to investigate the association between occurrence of the disease and some special condition or set of conditions. This is primarily a statistical process of ascertaining the frequency of the disease in two or more populations separated with respect to the particular condition. The association may be so obvious that no exact statistical expression is necessary, as, for instance, the association between the occurrence of a localized epidemic of measles and contact with a prior case. Or again, it may relate not to two, but to a considerable number of groups; and the primary difference' between these groups may be not in the existence or non-existence of the condition in question, but in its frequency. The establishment of associations in the more complex relations which often exist may be an intricate statistical procedure, yet the principle remains always the same; and in a very large proportion of important epidemiological investigations quite simple statistical methods will be adequate, and judgment of the statistical significance of the associations found will not be very difficult. Much greater difficulty will usually be found in securing groups which are actually equivalent with respect to conditions other than the one under investigation, or in making proper allowances for such other differences as exist.
(2) Almost invariably, in epidemiological studies, any single association which may be found is checked by its relation to a number of other associations and special circumstances, which will confirm or modify the significance of the single fact. For example, in a milk-borne epidemic of typhoid fever, the primary fact which associates the milk supply with the epidemic will probably be a much higher frequency of the disease in families which receive their supply from this source than in the rest of the population. Other related facts may be: that within these families there is a higher incidence of cases among those who drink milk freely than among those who use it sparingly; that the cases have occurred in such time relation to each other as suggests nearly simultaneous infection; and that a dairy employee, handling this particular milk supply, has developed typhoid fever some two or three weeks previously. Such a series of facts obviously has a more definite significance than any single one of the facts by itself. Not only in the investigation of epidemics, but quite generally in all epidemiological studies, the evidence will eventually consist of a series of facts which are related to each other, some being associations which are readily expressed statistically, and some being data of a different order. It is in the interrelation of the facts that epidemiological skill is needed.
(3) The interpretation, in an epidemiological sense, of any association which may be found in the local occurrence of a disease, always requires that the facts be related to the whole theory of the disease. The process of relating the special facts in a particular instance to the broader epidemiology of the infection .is usually implied rather than expressed in the actual presentation of studies which refer to diseases of well-known causation; but it is just as necessary in the explanation today of a local outbreak of typhoid fever, or diphtheria, or smallpox, as it was in Snow's explanation of the relation of cholera to water supplies in London.
The opinion is more or less prevalent that inferences based upon epidemiological argument cannot be truly conclusive, because the evidence is purely circumstantial. Such opinion has frequently failed to take account of the whole mass of evidence, and to follow the argument which is necessarily built up step by step in a somewhat complex and perhaps tedious way. Given sufficient scope and accuracy of observations, a conclusion as to the nature and spread of a disease may often be established quite firmly by circumstantial evidence well in advance of experimental confirmation. Moreover, many problems of disease transmission which are highly important from the standpoint of prevention, are such that can be solved only by investigation of this kind. The weakness in conclusions drawn from circumstantial studies is usually chargeable not to basic defects in the methods of investigation, but more often to paucity or inaccuracy of data, or to faults of logic in their interpretation.
REFERENCES
Budd, William: Typhoid Fever, its Nature, Mode of Spreading and Prevention, London, Longmans Green and Co., 1873.
Carter, H. R.: The Mechanism of the Spontaneous Elimination of Yellow Fever from Endemic Centers, Ann. Trop. Med. and Parasitol. 13:299, 1919-20.
d 'Herelle, F.: Immunity in Natural Infectious Diseases, English Edition, Baltimore, Williams & Wilkins Co., 1924.
Greenwood, M., Newbold, E. M., Topley, W. W. C., and Wilson, J.: On the Mechanisms by which Protection against Infectious Disease is Acquired in "Natural" Epidemics, J. Hygiene, 25: 336, 1926.
Hirsch, August: Handbook of Geographical and Historical Pathology, London, New Sydenham Society, 1883.
Snow, John: Continuous Molecular Changes, London, J. Churchill, 1853.
Snow, John: On the Mode of Communication of Cholera, London, J. Churchill, 1855.
Webster, Leslie T.: Experiments on Normal and Immune Mice with a Bacillus of Mouse Typhoid, J. Exper. Med. 36: 71, 1922.
Webster, Leslie T.: Microbic Virulence, and Host Susceptibility in Mouse Typhoid Infection, ibid. 37: 231, 1923."
Webster, Leslie T.: Microbic Virulence, etc., III, The Immunity of a Surviving Population, ibid. 39:129, 1924.
Wernstedt, W i 1 h e 1 m : Epidemiologische Studien ueber die zweite grosse Poliomyelitisepidemie in Schweden. 1911-1913. Ergeb. d. inn. Med. u. Kinderhlk., Berlin, 26:248, 1924.
Source: Wade H. Frost. Epidemiology. In: Public Health - Preventive Medicine from Nelson Loose-Leaf System. New York: Thomas Nelson & Sons, 1927